If you have been told you have endometriosis — or if you have spent years having your painful periods dismissed as normal — this article is for you. Endometriosis is a serious, complex, inflammatory condition that affects roughly 1 in 10 women of reproductive age worldwide. It is also one of the most poorly understood conditions in mainstream medicine, which is why so many people suffer for years before getting an accurate diagnosis and a real treatment plan.
I want to give you a thorough, honest picture of what endometriosis is, what drives it, and what a genuinely comprehensive management strategy looks like — one that includes both appropriate medical care and the nutritional and lifestyle interventions that can make a real difference in symptoms, inflammation, and quality of life.
What Endometriosis Actually Is — and What It Is Not
You will often hear endometriosis described as "the endometrium growing outside the uterus." This description is widespread, but it is an oversimplification that does not quite capture what is happening. The tissue found in endometriosis lesions is similar to the endometrial lining, but it is not identical. It behaves differently from normal endometrial tissue — it does not respond to hormonal signals in quite the same way, it is more invasive, and it triggers a distinct inflammatory response that normal endometrium does not.
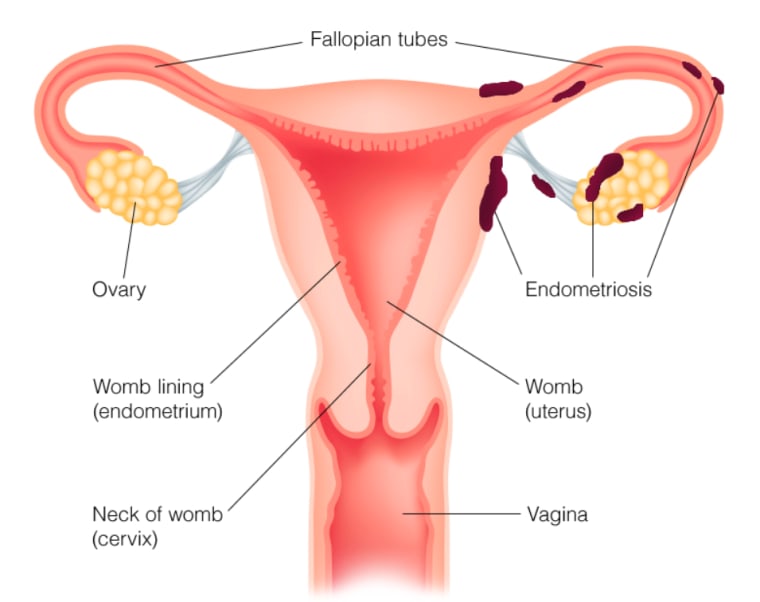
More precisely, endometriosis is a complex, inflammatory disease characterized by the growth of endometrial-like tissue outside the uterus. This tissue most commonly implants in the peritoneal cavity — the space surrounding the abdominal organs — but it can also grow on the fallopian tubes, ovaries, bowel, bladder, and in rare cases even on the lungs and diaphragm. Wherever it lands, this tissue behaves like endometrium in one critical way: it responds to the hormonal fluctuations of the menstrual cycle, swelling and breaking down each month. But unlike the uterine lining, it has nowhere to go. The result is chronic inflammation, scar tissue, adhesions, and the kind of pain that can be genuinely debilitating.
Endometriosis is currently only definitively diagnosed via laparoscopic surgery — ideally performed by a skilled excision surgeon. Other screening tools like transvaginal ultrasound, pelvic exams, and MRI can provide useful information, but they cannot confirm endometriosis the way a surgical biopsy can. This is one of the reasons diagnosis takes so long.
The Stages of Endometriosis — and Why Staging Does Not Tell the Whole Story
Endometriosis is classified in four stages:
- Stage 1 (Minimal): Small, isolated implants on or near the pelvic organs, with little or no scar tissue.
- Stage 2 (Mild): More implants, somewhat deeper, with some adhesions.
- Stage 3 (Moderate): Multiple deep implants, small cysts on one or both ovaries (endometriomas), and more significant adhesions.
- Stage 4 (Severe): Many deep implants, large endometriomas, and dense adhesions between the pelvic organs.
Here is the part that surprises most people: staging does not predict symptom severity. Someone with Stage 1 endometriosis can be in excruciating pain, while someone with Stage 4 might not find out they have the condition until they experience difficulty conceiving. This is because the stage does not reflect where the lesions are located relative to pain-sensitive nerves, nor how deeply they have infiltrated surrounding tissue. A small lesion near a nerve cluster can be far more painful than a large one in a less sensitive location.
There are also three recognized subtypes: superficial peritoneal endometriosis (the most common), deep infiltrating endometriosis, and ovarian endometriomas (cysts). A person can have more than one subtype simultaneously, which adds further complexity to diagnosis and treatment.
Where It Grows and How Symptoms Manifest
The location of endometriosis lesions shapes what symptoms a person experiences. Lesions on the bowel or intestines can cause significant GI dysfunction — constipation, diarrhea, bloating, and pain with bowel movements. Lesions on the bladder cause painful urination and may be mistaken for recurrent urinary tract infections. Lesions on the ovaries form cysts that cause pelvic pressure and impact fertility. Deep infiltrating endometriosis around the uterosacral ligaments is a common driver of severe menstrual pain and painful sex. The diversity of symptom presentations is one reason why endometriosis is so often missed or misattributed to IBS, bladder conditions, pelvic floor dysfunction, or just "bad periods."
Symptoms: What to Look For
The symptom picture for endometriosis can vary considerably from person to person, but the most common include:
- Severe dysmenorrhea: Period cramps that are significantly worse than typical, often disrupting daily life for one or more days. This is endometriosis' most hallmark symptom.
- Pelvic pain throughout the cycle: Pain that is not limited to menstruation — it can occur at ovulation, throughout the luteal phase, or even chronically.
- Dyspareunia: Pain during or after sex, often described as deep, aching, or stabbing. This is especially common when endometriosis affects the uterosacral ligaments or the cul-de-sac behind the uterus.
- Heavy or prolonged periods: Cycles lasting longer than seven days, or flow that is notably heavy.
- GI symptoms: Bloating (sometimes called "endo belly"), nausea — especially during menstruation — constipation, diarrhea, and pain with bowel movements.
- Debilitating fatigue: A level of exhaustion disproportionate to what lifestyle factors alone would explain, often worsening around menstruation.
- Infertility: Endometriosis is estimated to affect 30–50% of women with infertility. The mechanisms are multiple: adhesions can block the fallopian tubes, inflammation can impair egg quality, and endometriomas can damage ovarian reserve.
- Depression and anxiety: Mood changes, particularly worsening depression or anxiety in the luteal phase, are common — partly due to chronic pain and partly due to the systemic inflammatory state.
It is also worth knowing that endometriosis is frequently a condition whose symptoms begin at the very start of menstruation during puberty. It is, in fact, the leading cause of painful periods in adolescents. If you have had severe cramps since your very first period, that history is clinically relevant.
The Diagnostic Delay Problem
On average, it takes 7 to 10 years from the onset of symptoms to an endometriosis diagnosis. This is one of the most striking statistics in women's health, and it reflects a persistent problem: pain in women is routinely minimized, normalized, and dismissed. Women with endometriosis are frequently told their pain is "just bad periods," prescribed hormonal birth control without investigation, or sent home from the emergency room with pain medication and no answers.
The delay matters not just because of the years spent suffering without answers, but because endometriosis is a progressive condition. Left unmanaged, adhesions can spread, affecting fertility, bowel function, and bladder function. The earlier it is identified and addressed — both medically and through lifestyle interventions — the better the long-term outcomes.
If you recognize your symptom pattern in what I have described above and you have not been properly evaluated, please advocate for yourself. Ask for a referral to a gynecologist with specific expertise in endometriosis. Ideally, look for a surgeon who specializes in excision surgery (more on that below).
Root Causes: What Actually Drives Endometriosis
Endometriosis is not fully understood — there is ongoing research into why some women develop it. What is clear is that it is not a simple hormonal condition, despite often being characterized that way. Multiple mechanisms are at play.
Estrogen dependence and estrogen dominance
Endometriosis is an estrogen-dependent disease. The endometrial-like lesions respond to estrogen, which drives their growth and the associated inflammation. This means that anything contributing to estrogen dominance — excess estrogen, insufficient progesterone, impaired estrogen clearance — feeds the condition. Poor liver function, constipation, gut dysbiosis, and a high toxic burden can all impair the body's ability to break down and excrete estrogen efficiently, allowing it to recirculate and drive lesion activity.
Immune system dysfunction
There is a growing body of evidence that endometriosis has almost all the hallmarks of an autoimmune disease. It frequently co-occurs with other autoimmune conditions — including celiac disease, lupus, rheumatoid arthritis, Sjogren's syndrome, multiple sclerosis, and inflammatory bowel disease. In endometriosis, the immune system fails to recognize and clear the misplaced tissue, and the chronic inflammatory response it mounts creates a feedback loop that worsens the disease over time. High numbers of macrophages and mast cells accumulate in the peritoneal cavity and within lesions, contributing significantly to pain and tissue damage.
Chronic systemic inflammation
Systemic inflammation is both a cause and a consequence of endometriosis. An inflammatory diet, blood sugar dysregulation, gut permeability, and chronic stress all amplify the inflammatory environment in which endometriosis thrives. Reducing the total inflammatory burden on the body is one of the most impactful things a person can do to manage symptoms.
Gut microbiome disruption ("the endo dysbiome")
The gut connection to endometriosis is significant. Small intestinal bacterial overgrowth (SIBO) is a common comorbidity — partly because endometriosis can directly infiltrate the bowel and alter intestinal motility and bacterial populations. Many people with endometriosis are diagnosed with IBS before they ever get an endometriosis diagnosis. The gut microbiome also plays a critical role in estrogen metabolism: dysbiotic gut bacteria produce an enzyme called beta-glucuronidase that reactivates processed estrogen in the colon and allows it to be reabsorbed into circulation — directly feeding the estrogen-driven aspects of the disease.
Environmental toxins and xenoestrogens
Exposure to endocrine-disrupting chemicals — found in conventional pesticides, plastics, personal care products, and non-stick cookware — mimics estrogen in the body, contributing to the estrogenic load that drives endometriosis. Reducing xenoestrogen exposure is a meaningful, actionable part of a management strategy.
Genetics
Endometriosis has a genetic component. Women with a close relative who has endometriosis are significantly more likely to develop it themselves. In female twins, both are more likely to have the condition if they are identical. That said, genes are not destiny — diet, lifestyle, and environmental exposures all influence whether and how severely the condition manifests.
The Natural Protocol: What Can Actually Help
Let me be direct before going into this: natural approaches to endometriosis can meaningfully reduce symptoms, lower inflammation, support hormonal balance, and improve quality of life. They do not, however, remove endometriosis tissue. Surgery — specifically excision surgery — is the only way to physically remove lesions. The natural protocol I am describing works best as a complement to appropriate medical care, not a replacement for it.
With that said, these interventions are genuinely powerful. Many women with endometriosis see dramatic improvements in pain, bloating, fatigue, and cycle regularity when they implement a comprehensive approach.
Anti-inflammatory nutrition
Diet is one of the most impactful levers available for managing endometriosis. The goal is to reduce systemic inflammation and the total estrogenic burden in the body. This means:
- Eliminating the major inflammatory drivers: Gluten, dairy, refined sugar, alcohol, and conventionally raised meat (which carries hormone residues and inflammatory omega-6 fatty acids) are the foods most consistently associated with worsened endometriosis symptoms in clinical practice. Many women with endometriosis also have undiagnosed celiac disease or non-celiac gluten sensitivity — and the overlap between endometriosis and celiac disease is well documented.
- Emphasizing omega-3 fatty acids: Fatty fish (salmon, sardines, mackerel), flaxseeds, chia seeds, and walnuts provide EPA and DHA, which directly counter the prostaglandin-driven inflammation responsible for cramping and pain.
- Loading up on colorful vegetables: A broad array of vegetables — particularly deeply colored ones rich in antioxidants — reduces oxidative stress, supports immune function, and provides fiber for healthy estrogen excretion.
- Prioritizing fiber: Adequate fiber (25–35g daily) is essential for binding estrogen in the gut and ensuring it is excreted rather than reabsorbed. Legumes, seeds, and vegetables are all excellent sources.
- Cruciferous vegetables for estrogen metabolism: Broccoli, kale, cabbage, Brussels sprouts, and cauliflower contain indole-3-carbinol (I3C) and DIM, which support the liver's ability to metabolize estrogen down the less inflammatory 2-OH pathway. Aim for at least one to two servings daily.
Estrogen dominance protocol
Beyond diet, actively supporting estrogen clearance is essential. This involves optimizing liver detoxification pathways, ensuring healthy bowel transit time, and reducing the estrogen recycling that happens when beta-glucuronidase-producing bacteria are present in the gut. The cruciferous vegetable compounds mentioned above — and their supplemental equivalents DIM and I3C — directly support phase 1 liver estrogen metabolism. Calcium D-glucarate (500–1000 mg daily) addresses the gut end of estrogen clearance by inhibiting beta-glucuronidase. Liver support herbs like milk thistle and dandelion root support the downstream clearance steps. For a thorough review of how these compounds work, see the article on DIM and I3C.
Gut healing
Given the profound gut-endometriosis connection, addressing gut health is non-negotiable. This means reducing gut permeability through elimination of food sensitivities, supporting the mucosal lining with nutrients like L-glutamine and zinc, and working on the microbial imbalances — including SIBO — that perpetuate both GI symptoms and estrogen recirculation. A good probiotic (look for multi-strain formulas containing Lactobacillus and Bifidobacterium species) supports a healthier gut microbial environment and can directly influence estrogen metabolism and immune regulation.
Castor oil packs
One of the oldest and most consistently beneficial therapies for endometriosis-related pelvic pain is regular use of castor oil packs over the lower abdomen. Castor oil is rich in ricinoleic acid, which has anti-inflammatory and analgesic properties. When applied topically with a warm pack, it stimulates the lymphatic system, increases circulation to the pelvic organs, helps soften scar tissue and adhesions, and supports the body's detoxification processes. Women with endometriosis consistently report meaningful reductions in pelvic pain and bloating with regular castor oil pack use. Apply the pack to the lower abdomen (below the navel) for 30–60 minutes, three to four times per week. Do not use during menstruation or during the luteal phase if you are trying to conceive.
Targeted supplements
Several supplements have specific evidence or strong clinical rationale for endometriosis:
- N-acetyl cysteine (NAC): One of the most exciting supplements for endometriosis. A randomized controlled trial found that women taking NAC (600 mg three times daily, three days per week) experienced significant reductions in endometrioma size and pain — with a meaningful number choosing to decline surgery after completing the protocol. NAC works by reducing oxidative stress, supporting glutathione production, and directly targeting the inflammation within lesions.
- Magnesium: Magnesium glycinate or malate (300–400 mg daily) reduces prostaglandin production and muscle tension, directly targeting the cramping and pelvic floor tightness associated with endometriosis pain. Most women are deficient.
- Omega-3 fatty acids: A high-quality fish oil (EPA + DHA, 2–3 g combined per day) reduces the inflammatory prostaglandins (PGE2) that drive pain and promotes the production of anti-inflammatory prostaglandins instead.
- Vitamin D: Vitamin D has significant immune-modulating and anti-inflammatory effects. Low vitamin D is associated with worse endometriosis symptoms. Get your levels tested and aim for 50–80 ng/mL. Many women need 2,000–5,000 IU daily to reach and maintain this range.
- Zinc: Zinc supports immune function, reduces prostaglandin production, and is often depleted in women with endometriosis. Zinc bisglycinate at 15–30 mg daily is a well-absorbed form.
- Alpha lipoic acid (ALA): A powerful antioxidant that reduces oxidative stress in the peritoneal environment and has anti-inflammatory effects relevant to endometriosis.
- Curcumin: The active compound in turmeric has potent anti-inflammatory and anti-estrogenic effects. Research suggests it can inhibit the growth and invasiveness of endometriotic lesions. Look for a high-bioavailability form (with piperine or in a phospholipid complex). 500–1000 mg daily.
- Probiotics: As noted above, supporting the gut microbiome is central to endometriosis management. A broad-spectrum probiotic taken daily supports estrogen clearance, reduces gut inflammation, and supports immune function.
- DIM and I3C: As part of the estrogen metabolism support protocol. See the dedicated article on DIM and I3C for full dosing guidance.
Progesterone support
Because endometriosis is estrogen-driven, supporting progesterone is the natural counterbalance. Adequate progesterone — produced only after ovulation — opposes estrogen's proliferative effects. Supporting ovulation through blood sugar stabilization, stress management, and thyroid optimization is the foundational approach. Vitex (chasteberry) can support the LH surge and progesterone production in the luteal phase in some women, though it should be used thoughtfully and is not appropriate for everyone. In some cases, bioidentical progesterone cream (topical, luteal phase only) is worth discussing with a knowledgeable practitioner.
Reducing xenoestrogen exposure
Environmental estrogens add to the total estrogenic load in the body and feed estrogen-dependent endometriosis. Practical steps include: switching to glass or stainless steel food storage (avoiding BPA and phthalates in plastic), choosing organic produce for the most pesticide-heavy items, using natural personal care and cleaning products, and avoiding synthetic fragrances, which often contain endocrine disruptors. These changes compound over time and reduce the burden on the liver and lymphatic system.
Stress reduction and nervous system support
Chronic stress elevates cortisol, which dysregulates the immune system and amplifies inflammation — both directly relevant to endometriosis. HPA axis dysregulation is common in women with this condition. Prioritizing sleep, incorporating parasympathetic nervous system practices (breathwork, gentle yoga, time in nature), and addressing major life stressors is not soft advice — it has direct biological relevance to immune regulation and pain sensitivity.
Not sure where to start with your symptoms?
Take the free Hormone Health Assessment to get a personalized protocol based on your specific cycle symptoms and health history. It takes a few minutes and gives you a clear, prioritized starting point.
Take the Free Assessment →Surgery: When It Is Appropriate and Why Excision Matters
Surgery is an important part of endometriosis management, and for many women it is necessary — particularly when lesions are extensive, when an endometrioma is affecting ovarian reserve, or when conservative management has not provided adequate relief. I want to be direct about this: natural approaches cannot remove endometriosis tissue. Surgery can.
But not all surgery for endometriosis is equal — and this is a critical distinction.
Ablation (also called "burning" or "fulguration") involves burning or vaporizing the surface of endometriosis lesions. It is faster and more widely available. The problem is that it does not remove the full depth of the lesion, leaving the root behind. For superficial lesions, ablation may provide temporary relief, but for deep infiltrating endometriosis, it is largely ineffective and symptoms often return within months.
Excision surgery involves surgically cutting out the entire lesion, including its root and the surrounding affected tissue. This is the gold standard for endometriosis treatment. Studies consistently show higher rates of pain relief, longer symptom-free intervals, and lower recurrence rates with excision compared to ablation. If you are going to have surgery, it is worth seeking out a surgeon who specializes in excision — they exist in most countries but may require travel or advocacy to access.
Signs that surgery may be warranted include: endometriomas present on ultrasound, severe symptoms not responding to conservative management, documented fertility impairment, or suspected bowel or bladder involvement. These conversations should happen with a gynecological specialist who has genuine expertise in endometriosis — not a general gynecologist who does occasional laparoscopies.
A Note on Balance
Endometriosis is a serious condition that deserves serious, coordinated care. The natural protocol described here is genuinely impactful — I have seen women with endometriosis transform their quality of life through nutrition, targeted supplementation, castor oil packs, and gut healing. These interventions reduce inflammation, lower the estrogenic load, support immune function, and decrease pain. They are not optional extras.
But they work best alongside — not instead of — appropriate medical care. If you have not been properly evaluated, please get a proper diagnosis. If surgery is warranted, find an excision specialist. Natural and medical approaches are most powerful when used together. You deserve a team that takes your symptoms seriously and supports you with the full range of tools available.