If you grew up in the 1980s or 1990s, you were almost certainly told that cholesterol was the enemy. Eggs were suspect. Butter was dangerous. Fat-free was the goal. And cholesterol — well, cholesterol was the villain at the center of the whole story.
Here's the problem: that story was wrong. And for women especially, the consequences of decades of fat-phobia and cholesterol fear have been significant. Because cholesterol is not a dietary mistake. It is, quite literally, the raw material your body uses to build its most important hormones.
Without adequate cholesterol, you cannot make enough estrogen. You cannot make enough progesterone. Your testosterone will suffer. Your cortisol regulation will suffer. Your entire hormonal cascade depends on having enough of this molecule circulating in your body. And yet millions of women — eating low-fat diets, taking cholesterol-lowering medications, or simply never questioning the dominant nutritional narrative — are operating with a deficiency that shows up in their cycles, their moods, their libido, and their energy.
It's time to set the record straight.
Cholesterol Is the Mother of All Steroid Hormones
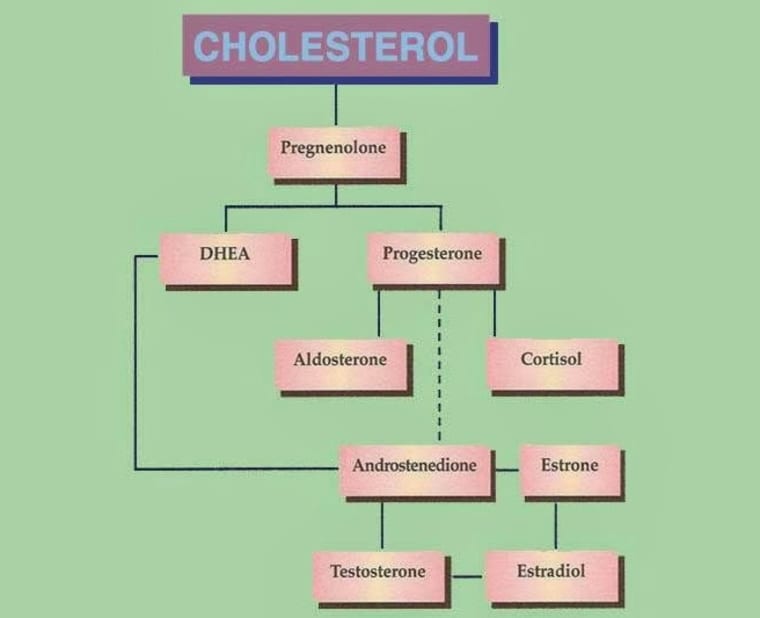
To understand why cholesterol matters so much for hormonal health, you need to understand how steroid hormones are made. Every single one of your sex hormones — estrogen, progesterone, testosterone, DHEA, and cortisol — belongs to a class called steroid hormones. And every steroid hormone in your body begins its life as cholesterol.
The process starts with something called the StAR protein (steroidogenic acute regulatory protein), which is produced by the StAR gene. This protein binds to cholesterol in the mitochondria of the adrenal glands and the gonads, initiating the first step of hormone synthesis. The result of this process is pregnenolone — often called the "mother hormone" or the "matriarch hormone" — because everything else flows downstream from it.
From pregnenolone, your body can produce:
- Progesterone — the luteal phase hormone essential for a healthy second half of your cycle, mood regulation, and sleep
- DHEA — the "fountain of youth" adrenal androgen that supports libido, fat metabolism, and immune function
- Cortisol — the stress-response hormone your body genuinely needs to survive
- Testosterone — critical for libido, muscle tone, bone density, and motivation in women
- Estrogen — the primary female sex hormone responsible for your cycle, cardiovascular health, bone density, and brain function
This entire cascade — from cholesterol to pregnenolone to every downstream steroid hormone — is why dietary fat is essential for hormone production. Your liver and intestines use healthy dietary fats to manufacture cholesterol. Restrict fat too aggressively, and you restrict the very substrate your hormonal system runs on.
What Happens When Cholesterol Is Too Low
Most of the public health conversation about cholesterol focuses on it being too high. Very little attention is paid to what happens when it's too low — and for women, the consequences can be profound.
When cholesterol levels drop below what the body needs for adequate steroid hormone synthesis, a range of hormonal symptoms can follow:
- Irregular or absent periods. If your body doesn't have enough raw material to produce adequate estrogen and progesterone, ovulation becomes inconsistent — and without ovulation, you don't get the hormonal rhythm that drives a regular cycle.
- Low progesterone. Progesterone is made primarily in the corpus luteum during the second half of the menstrual cycle, and it requires cholesterol as its direct precursor. Women on very low-fat diets often present with low progesterone — which shows up as a short luteal phase, PMS, anxiety, poor sleep, and spotting before the period.
- Low libido. Testosterone is closely linked to sexual desire in women, and testosterone production requires cholesterol. Low cholesterol is one of the underappreciated causes of a diminished sex drive.
- Mood issues and depression. Pregnenolone — that critical first hormone in the steroid cascade — has documented neuroprotective properties. It protects brain neurons, enhances memory and motivation, and has anti-inflammatory effects that support mental health. When the body doesn't have enough cholesterol to make sufficient pregnenolone, mood and cognitive function can suffer.
- Poor stress resilience. Cortisol is a steroid hormone derived from pregnenolone. Chronically low cholesterol can impair the adrenal glands' ability to mount an appropriate cortisol response, which paradoxically makes the body less able to handle stress — not more.
If you've been eating a low-fat diet for years and experiencing any combination of these symptoms, the connection is worth exploring with your practitioner.
The Truth About Dietary Cholesterol and Serum Cholesterol
One of the most persistent nutrition myths is that eating dietary cholesterol directly raises your blood cholesterol. The research does not support this — and for most people, eating cholesterol-rich foods has very little effect on serum cholesterol levels.
Here's why: your liver is the primary regulator of blood cholesterol. When you eat more dietary cholesterol, your liver compensates by making less of its own. When you eat less, the liver ramps up production. The body is remarkably good at maintaining its own cholesterol balance — and that's because it knows how essential this molecule is.
The foods that most strongly drive problematic changes in blood lipids are not eggs or butter — they are refined carbohydrates, excess sugar, and industrial seed oils (canola, corn, soy, cottonseed, sunflower). These foods promote the kind of chronic, systemic inflammation that actually damages blood vessels and distorts the balance between different lipid particles.
HDL, LDL, and What These Numbers Actually Mean for Hormones
When your doctor runs a cholesterol panel, you'll see numbers for HDL and LDL. These are not actually different types of cholesterol — they are lipoproteins, the transport vehicles that carry cholesterol through the bloodstream. HDL (high-density lipoprotein) carries cholesterol back to the liver for recycling. LDL (low-density lipoprotein) carries cholesterol out to tissues and cells throughout the body — including the adrenal glands and ovaries, where it is used to make hormones.
In the context of hormone production, LDL is not the villain it's been made out to be. It is the delivery mechanism that gets cholesterol to the cells that need it most. Extremely low LDL levels — something aggressively pursued through diet and medication in many patients — can leave the adrenals and gonads short on raw material for hormone synthesis.
HDL cholesterol, meanwhile, is consistently associated with better hormonal and cardiovascular outcomes. Regular physical activity, omega-3 rich foods, and minimizing processed seed oils are among the most reliable ways to support healthy HDL levels naturally.
Statins and Women's Hormones: What You Need to Know
Statins are among the most widely prescribed medications in the world, and they work by inhibiting HMG-CoA reductase — the enzyme the liver uses to synthesize cholesterol. For certain high-risk populations, their cardiovascular benefits are well established. But the impact on hormone production is rarely discussed with patients, particularly women.
Because statins lower the total pool of available cholesterol, they can reduce the substrate available for steroid hormone synthesis. Some women on statins report decreased libido, worsened mood, irregular cycles, and fatigue — symptoms that are consistent with downstream effects on the hormonal cascade. Muscle pain and weakness, common statin side effects, are also associated with impaired CoQ10 synthesis (statins block this pathway as well), which is important for mitochondrial energy production.
This is not an argument against statins for those who genuinely need them. It is an argument for informed conversations with your doctor — particularly if you are a premenopausal woman, if your cardiovascular risk is low to moderate, and if you are experiencing hormonal or energy-related symptoms after starting the medication.
The Best Foods to Support Healthy Cholesterol and Hormone Production
Supporting your body's cholesterol production doesn't mean eating recklessly. It means eating the kinds of whole, unprocessed fats that humans have consumed throughout history — and that the body is well equipped to use.
Eggs
Eggs are one of the most nutrient-dense foods available, and the yolk is particularly rich in cholesterol and fat-soluble nutrients. Pasture-raised eggs also have a significantly better omega-6 to omega-3 ratio than conventional supermarket eggs — one study found that free-range eggs had ratios around 1.5:1 compared to over 20:1 in conventional eggs. Egg yolks also contain choline, B vitamins, and vitamin D, all of which support hormonal health.
Liver and Organ Meats
Liver is arguably the single most nutrient-dense food you can eat. It is rich in cholesterol, fat-soluble vitamins A and D (both of which support hormone synthesis), vitamin K2, B vitamins including B12 and folate, and iron in its most bioavailable form. Even small amounts of liver weekly can meaningfully support hormonal nutrition.
Grass-Fed Butter and Ghee
Butter from grass-fed cows contains short and medium chain fatty acids that the body absorbs readily and uses efficiently, including for cholesterol production. It also contains fat-soluble vitamins and butyrate — a short chain fatty acid that supports gut lining integrity and reduces systemic inflammation. Ghee (clarified butter) offers the same benefits with most of the lactose removed, making it suitable for those with dairy sensitivities.
Fatty Fish and Shellfish
Salmon, sardines, mackerel, herring, and shellfish like oysters and mussels are rich in long-chain omega-3 fatty acids (EPA and DHA), which reduce the kind of systemic inflammation that impairs hormonal signaling. They also provide the building blocks for the anti-inflammatory prostaglandins that help regulate the menstrual cycle and reduce cramping.
Grass-Fed Beef and Lamb
Grass-fed and pasture-raised red meat has a dramatically better omega-6 to omega-3 fatty acid ratio than conventionally raised grain-fed animals. One study from North Dakota State University found that grass-fed bison had an omega-6 to omega-3 ratio of roughly 4:1, while grain-fed bison in feedlots had a ratio of 21:1. Quality matters enormously here.
Is your diet supporting your hormone production?
Hormonal imbalances rarely have a single cause — but nutrition is always part of the picture. The free Hormone Health Assessment looks at your cycle symptoms, energy, mood, and more to give you a personalized snapshot of what might be going on.
Take the Free Assessment →Inflammatory vs. Anti-Inflammatory Fats: The Critical Distinction
Not all fats support hormonal health equally. The distinction between inflammatory and anti-inflammatory fats is one of the most important concepts in nutritional hormone support — and it comes down largely to the balance between omega-6 and omega-3 fatty acids.
Both are essential fats that the body cannot manufacture on its own. But they have opposing effects on inflammation. Omega-6 fatty acids are precursors to pro-inflammatory prostaglandins (specifically PGE2), while omega-3 fatty acids are precursors to anti-inflammatory prostaglandins (PGE1 and PGE3). When the body has more omega-6 than omega-3, it tips toward a pro-inflammatory state.
Humans evolved consuming omega-6 and omega-3 in roughly a 1:1 ratio. In the modern Western diet, that ratio has shifted to somewhere between 10:1 and 20:1 in favor of omega-6 — driven largely by the widespread use of industrial vegetable oils (canola, corn, soy, sunflower, cottonseed) and the shift toward grain-fed rather than grass-fed livestock. The consequences include chronic systemic inflammation, worsened menstrual cramps, more severe PMS, and impaired hormonal signaling throughout the cycle.
Women with dysmenorrhea (painful periods) consistently show higher levels of PGE2 compared to women without menstrual pain. This inflammatory prostaglandin is at its highest in the first two days of the period — exactly when the pain is at its worst. Shifting the dietary fat balance toward more omega-3s and away from industrial omega-6 seed oils can significantly reduce this prostaglandin burden. This is also closely connected to blood sugar and insulin regulation, since inflammation impairs insulin sensitivity and vice versa.
The anti-inflammatory fats to prioritize include:
- Wild-caught fatty fish (salmon, sardines, mackerel, herring, anchovies)
- Algae oil (for those who don't eat fish)
- Walnuts, chia seeds, and flaxseeds (plant-based ALA that can be partially converted to EPA and DHA)
- Extra-virgin olive oil and avocados (monounsaturated fats with anti-inflammatory properties)
- Grass-fed butter and ghee (with a much healthier fatty acid profile than grain-fed dairy)
The fats to reduce or eliminate are industrial seed oils — the highly processed polyunsaturated oils that are unstable, prone to oxidation, and ubiquitous in processed foods and restaurant cooking. These are the true dietary drivers of chronic inflammation, and reducing them is one of the highest-leverage changes you can make for hormonal health.
Bringing It All Together
The fear of fat and cholesterol that dominated nutritional thinking for decades has left a legacy of hormonal disruption that we are still grappling with. The women who grew up eating fat-free yogurt, margarine, and skinless chicken breast — avoiding eggs and butter and anything that might raise their cholesterol — were not eating their way to health. In many cases, they were inadvertently depriving their bodies of the very raw materials needed to build a functioning hormonal system.
The fix is not complicated. Eat real, whole fats from quality sources. Prioritize eggs, liver, butter, fatty fish, and grass-fed meats. Reduce industrial seed oils and processed foods. Support your omega-6 to omega-3 balance. Give your body the cholesterol it needs to produce the pregnenolone that cascades into every steroid hormone your system depends on.
Your cycles, your mood, your libido, your energy — they are all downstream of this foundational nutritional truth. If you want to understand more about how hormones and metabolism interact, or why low progesterone is so common in women eating low-fat diets, those articles are a good next step.
Cholesterol isn't the villain. In the right context — which is the context of a whole-food diet and a body trying to produce its hormones — it's one of the most important molecules you've got.