Most conversations about blood sugar focus on diabetes, weight, and energy. What gets far less attention is the intimate, bidirectional relationship between blood sugar regulation and your menstrual cycle — a relationship that plays out every single month whether you are aware of it or not.
On one side: your sex hormones — estrogen, progesterone, and androgens — directly influence how sensitive your cells are to insulin across each phase of the cycle. On the other side: blood sugar dysregulation and chronically elevated insulin are among the most powerful disruptors of the hormonal cascade that governs ovulation, cycle regularity, and everything from your skin to your mood in the days before your period.
This article covers both directions of that relationship in full, draws on research and clinical experience, and gives you a practical, evidence-based protocol for stabilizing blood sugar in a way that supports your hormones throughout your entire cycle.
The Bidirectional Relationship: It Works Both Ways
The connection between blood sugar and hormonal health is not a one-way street. It is a feedback loop, and both directions matter:
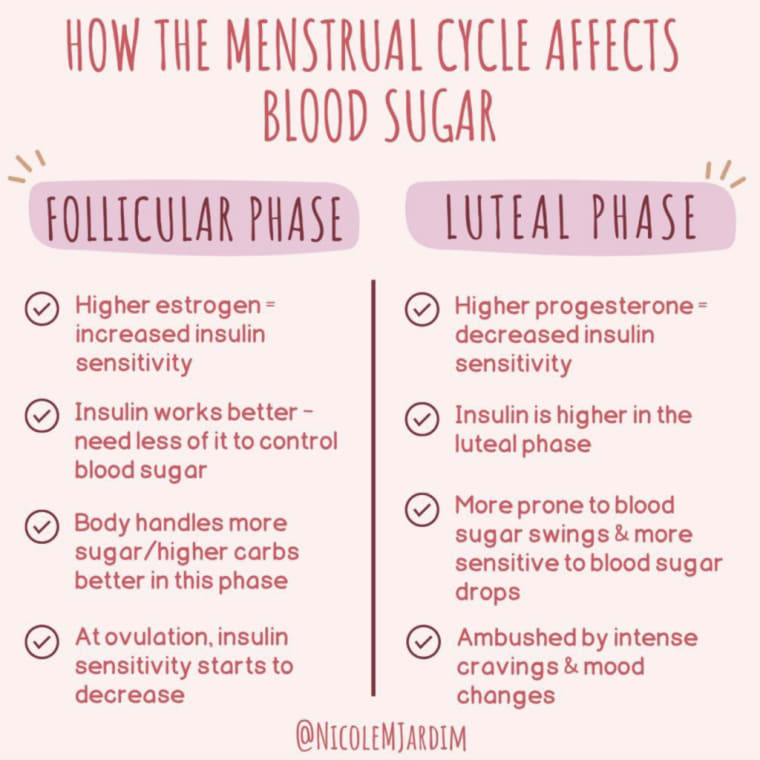
- Your hormones affect blood sugar. Estrogen improves insulin sensitivity. Progesterone — particularly in the luteal phase — reduces it. These shifts happen every cycle and directly influence your cravings, energy stability, and how your body responds to the foods you eat at different times of the month.
- Your blood sugar affects your hormones. Chronically elevated blood sugar and insulin trigger a downstream cascade that raises androgens, suppresses ovulation, creates estrogen dominance, drives cortisol dysregulation, and can push susceptible women toward PCOS.
Understanding both sides changes how you approach eating, supplementation, and lifestyle support — and it explains why what works well for your body in the first half of your cycle may feel completely different in the second half.
How Insulin Sensitivity Shifts Across Your Cycle
Your cycle is not a flat hormonal landscape — it is a dynamic sequence of shifting estrogen, progesterone, LH, and FSH, and each of these hormones interacts with insulin in specific ways. Here is what happens at each phase:
Follicular Phase (Days 1–14)
Rising estrogen improves insulin sensitivity. Your cells respond more readily to insulin, blood sugar is more easily stabilized, and you tend to have better energy and fewer cravings. This is the best time of your cycle to enjoy foods that spike blood sugar without as pronounced a consequence.
Ovulation (Around Day 14)
Insulin sensitivity is near its peak as estrogen surges. Many women feel their sharpest, most energetic, and most metabolically resilient right around ovulation — this is partly why. Blood sugar tends to be most stable, and your body handles carbohydrates efficiently.
Luteal Phase (Days 15–28)
After ovulation, estrogen drops and progesterone rises. Progesterone appears to reduce insulin sensitivity, making cells less responsive to insulin's signal to absorb glucose. This is when blood sugar swings — from highs to lows — become more pronounced, cravings intensify, and the same foods that felt fine in the follicular phase can now cause energy crashes, mood swings, and anxiety.
Menstruation (Days 1–5)
As estrogen and progesterone both fall, insulin sensitivity begins to recover. Many women notice cravings ease after their period begins and energy gradually stabilizes — this is the physiology reasserting a more insulin-sensitive baseline as the follicular phase restarts.
This cycling of insulin sensitivity is not a flaw — it is physiology. But it becomes clinically important when blood sugar is already dysregulated, because the luteal reduction in insulin sensitivity amplifies the consequences of blood sugar instability significantly. PMS, mood swings, cravings, fatigue, acne, and disrupted sleep in the second half of the cycle are all, in part, downstream effects of reduced insulin sensitivity interacting with an unstable blood sugar baseline.
I always recommend phase-specific dietary adjustments for this reason: leaning into more protein and fat in the luteal phase, enjoying naturally sweeter foods more freely in the follicular phase, and never trying to apply a one-size approach across all four phases.
How Blood Sugar Dysregulation Disrupts Your Hormonal Cascade
This is the direction of the relationship that causes the most long-term hormonal damage — and the one that is most correctable with targeted intervention.
Insulin, Androgens, and the PCOS Connection
The ovaries have insulin receptors, and they are extremely sensitive to chronically high insulin levels. When insulin is elevated — either from chronic overconsumption of refined carbohydrates or from underlying insulin resistance — several things happen that collectively drive androgen excess:
- High insulin stimulates LH production in the pituitary gland, and amplifies LH's effect on the ovaries. This combination signals the ovaries to produce excess androgens — specifically testosterone — instead of following the normal follicle maturation sequence that produces estrogen and leads to ovulation.
- High insulin suppresses sex hormone binding globulin (SHBG) — the protein made by the liver that binds testosterone and keeps it inactive in the bloodstream. Less SHBG means more free testosterone circulating. More free testosterone means more androgen-driven symptoms: irregular cycles, acne, oily skin, excess facial and body hair, and hair thinning on the scalp.
- High androgens cause further insulin resistance — creating a self-reinforcing vicious cycle that is difficult to break without directly addressing blood sugar.
The cascade runs like this: chronically elevated blood sugar → chronically elevated insulin → excess androgen production in the ovaries → suppressed SHBG → more free testosterone → PCOS symptoms → more insulin resistance. For women who are genetically predisposed to PCOS, this is frequently the underlying mechanism driving their diagnosis, regardless of body weight.
This is why blood sugar stabilization is not just a lifestyle recommendation for women with PCOS — it is often the most important single intervention available. No supplement protocol, no hormonal treatment, and no dietary tweak works as well as removing the insulin-androgen driver at the root.
Insulin, Aromatase, and Estrogen Dominance
Insulin resistance raises the activity of an enzyme called aromatase — the enzyme responsible for converting androgens (androstenedione and testosterone) into estrogens (estrone and estradiol). This means that chronically high insulin does not just raise androgens; it also creates excess estrogen, particularly estrone, which can contribute to estrogen dominance.
Estrogen dominance — when estrogen becomes chronically elevated relative to progesterone — disrupts the feedback loop between the brain and the ovaries. The hypothalamus reads high estrogen as a signal that follicle development is already underway, so it suppresses FSH. With FSH suppressed, follicles cannot develop normally. Ovulation becomes irregular. Without a corpus luteum forming at ovulation, progesterone is not produced for the second half of the cycle — which worsens estrogen dominance further. The cycle becomes a feedback loop of insufficiency.
Blood Sugar Spikes, Cortisol, and Progesterone Loss
Every significant blood sugar spike — and the reactive hypoglycemic crash that follows it — is registered by the body as a physiological stressor. The adrenal glands respond by releasing cortisol to raise blood sugar back up. In the short term, this works. But with frequent blood sugar instability, cortisol is being chronically triggered throughout the day.
Chronic cortisol activation depletes progesterone through the mechanism known as pregnenolone steal: your body's shared raw material for manufacturing steroid hormones gets redirected toward cortisol production at the expense of progesterone and other sex hormones. The downstream effects include:
- Short luteal phase and spotting before your period
- Anxiety, irritability, and low mood in the days before menstruation
- Disrupted sleep, particularly in the second half of the cycle
- Worsened PMS and PMDD symptoms
- Heavy or irregular periods from the resulting estrogen-progesterone imbalance
The Inflammatory Driver: Blood Sugar and Period Pain
Chronically elevated blood sugar and insulin create systemic, low-grade inflammation — damage to the endothelial cells lining blood vessels throughout the body, including the reproductive organs. This invisible inflammation is the same physiological response as a visible injury; it just happens internally and continuously when blood sugar is consistently high.
This inflammatory environment directly amplifies prostaglandin production at menstruation. Women with higher inflammatory loads have elevated levels of PGF2a — the prostaglandin responsible for uterine contractions, blood vessel constriction, and menstrual cramps. Reducing blood sugar dysregulation reduces this inflammatory background, which is one of the most reliable dietary routes to less painful periods.
Signs Your Blood Sugar May Be Affecting Your Cycle
Blood Sugar and Hormonal Symptoms to Watch For
- Intense cravings for sugar and carbohydrates in the week before your period
- Energy crashes in the mid-afternoon, especially in the luteal phase
- Feeling shaky, irritable, or foggy when meals are delayed ("hangry")
- Waking at night — particularly between 2 and 4am — due to blood sugar dropping
- Mood swings, anxiety, or tearfulness that worsen in the second half of your cycle
- Acne that flares around ovulation or before your period, often hormonal/cystic
- Irregular, absent, or anovulatory cycles (cycles without ovulation)
- Heavy or prolonged periods with clotting
- Spotting in the days before your period starts
- Oily skin, excess facial or body hair, or hair thinning on the scalp
- Weight gain or difficulty losing weight, particularly around the abdomen
- Needing coffee to function in the morning before eating
- Feeling worse on low-carb diets — extreme fatigue, worsened PMS, missing periods
If several of these symptoms are familiar, blood sugar dysregulation is very likely a contributing driver of your hormonal symptoms — even if you have never been diagnosed with prediabetes or insulin resistance. Functional blood sugar imbalance operates well below diagnostic thresholds and still creates significant downstream hormonal disruption.
The Complete Blood Sugar Balancing Protocol
The following protocol draws on the dietary principles, lifestyle interventions, and targeted supplementation that consistently produce the best results for women working on hormonal health through blood sugar stabilization. None of these are difficult in isolation — the power comes from applying them consistently and together.
Protein at Every Meal, Starting at Breakfast
A protein-rich breakfast within an hour of waking is one of the most important single interventions for blood sugar and hormonal health. Eating only coffee in the morning prolongs the overnight fast, forcing the adrenal glands to produce cortisol to maintain blood glucose. This starts a cycle of cortisol activation that runs all day. Aim for at least 25–30 grams of protein at breakfast — eggs, Greek yogurt, smoked salmon, a protein-rich smoothie — and include protein with every meal and snack throughout the day.
Protein slows the digestion and absorption of carbohydrates, blunts post-meal blood sugar spikes, and keeps insulin within a stable range throughout the day.
Never Eat Carbohydrates Alone
Every meal and snack should pair carbohydrates with protein, fat, and fiber. This is not about eliminating carbohydrates — it is about preventing the isolated glucose spike that sends blood sugar and insulin surging, followed by the crash and the cortisol response that follows. A banana on its own is a different metabolic event from a banana with almond butter. Sweet potatoes are different from sweet potatoes alongside eggs and greens.
Fiber First — Eat in the Right Order
The order in which you eat the components of a meal meaningfully affects your blood sugar response. Starting with fiber — a salad, roasted vegetables, raw crudités — before the protein and fat, and eating starchy or sugary components last, significantly reduces post-meal glucose spikes. Research on meal sequencing consistently shows this effect: the same foods eaten in a different order produce measurably different insulin responses.
Add a tablespoon of apple cider vinegar diluted in water before meals — or try a quality herbal "metabolic vinegar" tincture before your largest meal of the day — both have evidence for reducing post-meal glucose levels.
Movement After Meals
A 10–20 minute walk after eating is one of the most powerful tools for blood sugar management available. When muscles contract, they absorb glucose from the bloodstream independently of insulin — which means post-meal movement dramatically reduces blood sugar spikes and keeps insulin from spiking high in response. If a walk is not possible, a few minutes of squats, jumping jacks, or light housework achieves a similar effect. This single habit can be more impactful than many supplements.
Sleep and Blood Sugar
Sleep deprivation is a direct cause of insulin resistance. Even one night of poor sleep reduces insulin sensitivity the following day. The mechanism is bidirectional: poor sleep raises cortisol and ghrelin (hunger hormone), which drives cravings for sugar and refined carbohydrates the next day. Simultaneously, blood sugar instability — including nocturnal hypoglycemia from reactive blood sugar drops — disrupts sleep, waking women up between 2 and 4am as cortisol rises to compensate.
Prioritizing 7–9 hours of consistent sleep is not a passive lifestyle choice for blood sugar — it is an active metabolic intervention. Eating a small protein-and-fat snack before bed (not carbohydrate-heavy) helps prevent the overnight drops that trigger this cortisol-waking pattern.
Stress and Blood Sugar
Every stress response — psychological or physical — triggers a cortisol release that raises blood sugar, even without eating. This is why women under chronic stress often find blood sugar management frustratingly difficult: the adrenals are continually producing glucose-raising cortisol regardless of what is on the plate. Managing stress load — through nervous system practices, reducing excessive exercise intensity during the luteal phase, and addressing gut and sleep issues — is part of a complete blood sugar stabilization approach.
Foods That Stabilize vs. Spike
Stabilizing: Non-starchy vegetables, leafy greens, cruciferous vegetables, berries, legumes, nuts, seeds, eggs, fatty fish, pastured meat and poultry, olive oil, avocado, sweet potatoes and other root vegetables (when paired with protein and fat), and cinnamon (which improves insulin sensitivity — aim for half to one teaspoon daily).
Spiking: Refined grains and flour products (white bread, pasta, crackers), added sugars in any form, fruit juices, sweetened beverages, ultra-processed snack foods, alcohol, and caffeine consumed alone on an empty stomach.
For sweeteners, monk fruit, stevia, erythritol, and allulose are all options that do not raise blood sugar and can replace conventional sugar when needed.
Get your personalized hormonal health protocol
Take the free Hormone Health Assessment — 30 questions about your cycle, symptoms, and lifestyle — and receive a tailored action plan built for your body.
Take the Free Assessment →Targeted Supplements for Blood Sugar and Insulin Balance
Several supplements have strong evidence for improving insulin sensitivity and supporting blood sugar regulation in the context of hormonal health. These work best as additions to the dietary and lifestyle foundation above, not substitutes for it.
Inositol (Myo-Inositol + D-Chiro-Inositol)
Inositol is a carbohydrate naturally present in the body that plays a central role in insulin signaling and ovarian function. It is the most researched supplement specifically for the blood sugar-hormonal health connection in women. Studies show inositol supplementation improves insulin sensitivity, lowers testosterone, reduces androgen-driven symptoms like irregular periods and hirsutism, improves egg quality, and helps restore ovulation in women with PCOS.
The two primary forms are myo-inositol and D-chiro-inositol. The body naturally maintains these in a 40:1 ratio (myo to D-chiro), and research supports supplementing in this same ratio. Products like Ovasitol by Theralogix provide 1,000mg myo-inositol plus 25mg D-chiro-inositol per dose, taken twice daily. For myo-inositol alone, 2–6 grams per day divided into 2–3 doses is the studied range. Inositol also has benefits for mood, anxiety, and perimenopausal metabolic health.
Magnesium
Magnesium is required for the proper function of insulin receptors — it activates the enzyme tyrosine kinase, which is essential for insulin receptor signaling. Without adequate magnesium, insulin receptors cannot work optimally, meaning blood sugar regulation suffers regardless of what else you do. Magnesium is chronically deficient in the majority of the population and is rapidly depleted by chronic stress, making it one of the most broadly relevant supplements for women with blood sugar and hormonal concerns.
Recommended dose: 300–400mg daily. Magnesium glycinate is well tolerated and well absorbed. Magnesium malate is particularly useful if musculoskeletal pain is also present. Take in the evening — magnesium also supports sleep quality, which supports insulin sensitivity the following day.
Berberine
Berberine is a natural plant compound that activates AMPK (adenosine monophosphate-activated protein kinase), an enzyme that triggers glucose breakdown and directly reduces insulin resistance. It is one of only a handful of compounds known to activate AMPK, and research consistently shows it improves fasting glucose, fasting insulin, and HbA1c in people with metabolic dysfunction. Recommended dose: 300–500mg once or twice daily with meals. Note that berberine should be used with caution if you are taking diabetes medications, antibiotics, antidepressants, or immune-suppressing drugs — always consult your healthcare provider. It is not appropriate during pregnancy or breastfeeding.
Chromium
Chromium is a trace mineral that enhances the action of insulin by potentiating insulin receptor signaling. Low chromium status is associated with impaired glucose tolerance and increased carbohydrate cravings. Chromium picolinate is the most bioavailable form. Typical doses studied for blood sugar support range from 200–1,000 mcg per day. It is particularly useful for women with pronounced sugar and carbohydrate cravings in the luteal phase.
Alpha Lipoic Acid (ALA)
Alpha lipoic acid is a powerful antioxidant that also improves insulin sensitivity and helps reduce oxidative stress in the blood vessels — the same endothelial damage that chronically high blood sugar creates. ALA supports glucose uptake into cells independently of insulin and has evidence for reducing fasting glucose and improving insulin sensitivity markers. Typical doses studied range from 300–600mg per day. It is also broadly anti-inflammatory and supports liver function, making it useful for women with estrogen metabolism concerns alongside blood sugar dysregulation.
Eating in Sync with Your Cycle
Given that insulin sensitivity shifts meaningfully across the four phases of the menstrual cycle, applying phase-specific dietary guidance is one of the most practical ways to work with your body rather than against it:
- Follicular and ovulatory phases: Higher insulin sensitivity means your body handles carbohydrates more efficiently. This is the time to enjoy naturally sweeter foods, whole fruit, and higher-carbohydrate meals, while still pairing them with protein and fat.
- Luteal phase: Reduced insulin sensitivity means blood sugar spikes are more pronounced and their hormonal consequences are amplified. Increase protein and healthy fat at every meal, reduce refined and high-glycemic carbohydrates, and prioritize blood sugar stabilizing practices (apple cider vinegar before meals, fiber first, post-meal movement) consistently through this phase.
- Menstruation: As insulin sensitivity begins to recover, focus on iron-rich and anti-inflammatory foods while continuing to stabilize blood sugar to reduce the prostaglandin-driven inflammation underlying cramps and fatigue.
This is not about restriction or perfection. It is about understanding that your body is not the same metabolic entity throughout the month — and that giving it what it actually needs at each phase is more effective than any fixed dietary rule applied uniformly all cycle long.