The luteal phase is arguably the most underappreciated part of your menstrual cycle. Most cycle conversations center on ovulation or your period itself — but what happens in the days between those two events matters enormously for how you feel, whether you can get pregnant, and whether your period actually shows up on time and without a lot of drama.
A short luteal phase is one of those issues that can quietly wreak havoc on your hormones for years before anyone identifies it. You might be spotting before your period, dealing with relentless PMS, struggling to conceive, or simply feeling "off" in the second half of your cycle — and no one has ever told you why. This article is here to change that.
What Is the Luteal Phase?
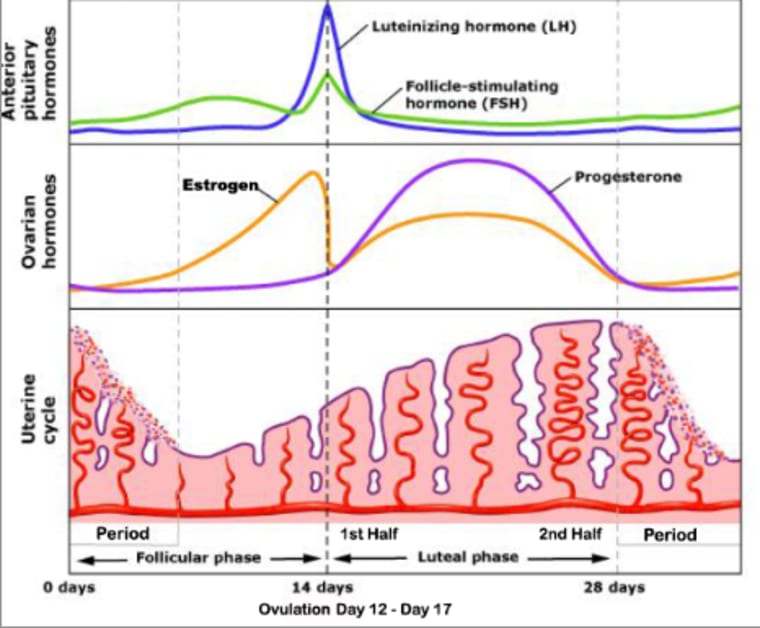
Your menstrual cycle has four phases: menstruation, the follicular phase, ovulation, and the luteal phase. The luteal phase begins the day after you ovulate and ends the day before your next period arrives. It is the second half of your cycle, and it is dominated by one very important hormone: progesterone.
Here is what actually happens during the luteal phase. When your ovary releases an egg at ovulation, the empty follicle transforms into a temporary endocrine gland called the corpus luteum. This remarkable little structure — which your body builds from scratch in under 24 hours — is what produces the bulk of your progesterone. It pumps out progesterone to thicken and stabilize the uterine lining in case a fertilized egg needs to implant. If no pregnancy occurs, the corpus luteum eventually breaks down, progesterone drops, and your period begins.
The length of your luteal phase depends entirely on how long the corpus luteum can maintain its progesterone production. When the corpus luteum is healthy and producing adequate progesterone, the luteal phase runs its full course. When it is not, you end up with a short luteal phase — and all the symptoms that come with it.
What Is a Normal Luteal Phase Length?
A healthy luteal phase typically lasts 11 to 17 days, with most people landing between 12 and 14 days. When your luteal phase falls within this range, it means your corpus luteum is producing enough progesterone to sustain the lining long enough for a potential pregnancy — or, if pregnancy does not occur, for a normal, well-timed period.
A luteal phase of 10 days or fewer is considered a short luteal phase. When it is 9 days or less, this is formally known as Luteal Phase Deficiency (LPD). At this length, there is not enough progesterone exposure to properly prepare the endometrium, and if a fertilized egg is traveling down the fallopian tube, it may not reach the uterus before the lining starts to shed.
One more thing worth knowing: because the length of the follicular phase (the first half of your cycle) varies from person to person and cycle to cycle, your total cycle length can vary — but your luteal phase tends to be relatively consistent once ovulation occurs. This means that even if you have a 26-day cycle or a 34-day cycle, your luteal phase should still be within that 11–17 day range. If it is not, something needs to be addressed.
Symptoms of a Short Luteal Phase

The symptoms of a short luteal phase are essentially the symptoms of low progesterone, because that is the underlying driver. Here is what to look for:
- Spotting 3 or more days before your period — this is one of the most telltale signs. When progesterone drops too quickly or was never high enough, the uterine lining begins to shed before your actual period. One to two days of brownish spotting before a period is usually fine; three or more days is a signal.
- PMS that starts early or feels excessive — mood swings, anxiety, overwhelm, irritability, cramps, bloating, breast tenderness, and headaches in the second half of your cycle are all signs that progesterone is not where it should be.
- Short cycles overall — if your total cycle is consistently under 25 days, it is very likely your luteal phase is too short.
- Difficulty getting or staying pregnant — a short luteal phase is a common factor in unexplained infertility and recurrent early miscarriage.
- Heavy or long periods — without enough progesterone to counter estrogen's stimulating effect on the uterine lining, the lining builds up excessively and then sheds heavily.
- Insomnia or poor sleep in the second half of your cycle — progesterone has a calming, sleep-promoting effect. When it is low, sleep often suffers.
- Period pain and cramping in the days before your period — progesterone is anti-inflammatory; when it drops prematurely, so does that natural buffer against pain.
How to Track Your Luteal Phase
You cannot fix a short luteal phase if you do not know you have one — and most people have no idea how long their luteal phase actually is. The good news is that tracking it is straightforward once you know what to look for.
The luteal phase begins the day after ovulation, so you first need to confirm when you ovulate. Here are the most reliable ways to do that:
- Basal Body Temperature (BBT) tracking — progesterone is a thermogenic hormone, meaning it raises your resting body temperature. After ovulation, you will see a sustained temperature shift of roughly 0.2°C upward that lasts for the rest of your cycle. The first day of this sustained rise is typically the day after ovulation.
- Cervical fluid monitoring — in the days leading up to ovulation, cervical fluid becomes clear, slippery, and stretchy (similar to raw egg white). After ovulation, progesterone causes it to become thick, tacky, or dry. The last day of this fertile-quality fluid is typically the day of or day before ovulation.
- LH testing strips — over-the-counter LH strips detect the luteinizing hormone surge that triggers ovulation. The LH surge typically starts 24–36 hours before ovulation, so tracking with these strips alongside BBT gives you the clearest picture.
Once you confirm your ovulation day, count forward to the first day of your next period. That number of days is your luteal phase. If it is consistently 10 days or less, you have a short luteal phase and this protocol is for you.
Get your personalized hormonal health protocol
Take the free Hormone Health Assessment — 30 questions about your cycle, symptoms, and lifestyle — and receive a tailored action plan built for your body.
Take the Free Assessment →What Causes a Short Luteal Phase?
A short luteal phase comes down to one fundamental issue: the corpus luteum is not producing enough progesterone to sustain the lining for the full required time. But there are several reasons why that might be happening, and identifying yours is key to fixing it.
Low Progesterone or Ovulatory Problems
Progesterone is an ovulation-dependent hormone — it is almost exclusively produced after ovulation, by the corpus luteum. So if you are not ovulating consistently, ovulating but with a weak or unhealthy corpus luteum, or not ovulating at all in some cycles, your progesterone production will be insufficient. The health of the follicle leading up to ovulation directly influences how well the corpus luteum performs afterward.
Nutrient Deficiencies
The ovaries are metabolically demanding organs — they require adequate vitamins, minerals, and antioxidants to produce healthy follicles and a well-functioning corpus luteum. Deficiencies in vitamin C, vitamin E, vitamin A, magnesium, and zinc are all associated with impaired corpus luteum function and lower progesterone production. Nutrient malabsorption (from gut issues) can compound this even when diet is good.
Chronic Stress
When you are under chronic stress, your body prioritizes survival hormones like cortisol — and cortisol competes with progesterone for the same hormone receptors. This means even if your progesterone levels are in a technically "normal" range on a lab test, high cortisol can block progesterone from getting into its receptors, producing symptoms of deficiency. Beyond receptor competition, prolonged stress can suppress the ovulatory process itself, lowering progesterone at the source.
Thyroid Dysfunction
The ovaries need thyroid hormone to function properly. Hypothyroidism (underactive thyroid) is strongly associated with luteal phase deficiency, short luteal phases, and low progesterone. High prolactin (which is often elevated in thyroid problems) also directly inhibits ovulation. If you have unexplained luteal phase issues, getting a full thyroid panel — including TSH, free T3, free T4, and thyroid antibodies — is worth doing.
Coming Off Hormonal Birth Control
After stopping hormonal birth control, it takes time for your hypothalamic-pituitary-ovarian axis to fully resume communication. During this re-regulation period, ovulation may be inconsistent, delayed, or result in weaker corpus luteum function — all of which can produce a short luteal phase. This is very common in the first 3–12 months post-pill, and it is absolutely addressable.
High Estrogen Relative to Progesterone
Even if your progesterone production is adequate in absolute terms, if your estrogen is elevated, the progesterone-to-estrogen ratio is off. These two hormones work like a seesaw. Estrogen stimulates uterine lining growth; progesterone stabilizes it. When estrogen dominates, the lining is overstimulated, and the effect of progesterone is diminished — producing symptoms that look exactly like low progesterone even when levels are technically fine on paper.
Gut Dysbiosis
An unhealthy gut microbiome produces endotoxins from harmful bacteria that can trigger an inflammatory response in ovarian tissue, directly impacting how well the ovaries function and how much progesterone the corpus luteum produces. Poor gut health also impairs estrogen detoxification, which feeds back into the estrogen-dominance problem described above.
The Full Protocol: How to Lengthen Your Luteal Phase
Here is the complete protocol I use with clients. It is built in layers — each step builds on the one before it — so please do not jump straight to the supplements and skip the foundations. The foundations are what actually make the supplements work.
Step 1: Confirm You Are Ovulating
Everything starts here. If you are not ovulating consistently, your body cannot produce adequate progesterone, full stop. Use BBT charting and cervical fluid monitoring to confirm whether you are ovulating each cycle. If you are not, that becomes the primary problem to address before anything else.
Step 2: Build a Hormone-Supporting Diet
Your ovarian function is only as good as the raw materials you are giving it. A nutrient-dense diet with adequate protein, healthy fats, fiber, and complex carbohydrates is non-negotiable for healthy follicles and corpus luteum function. Specific things to prioritize:
- Enough dietary fat — cholesterol is the precursor to all steroid sex hormones including progesterone. Very low-fat diets can suppress hormone production.
- Adequate fiber (25–35g daily) to support regular bowel movements, which is how your body clears metabolized estrogen. If estrogen builds up due to sluggish elimination, it tips the estrogen-progesterone balance in the wrong direction.
- Liver and other organ meats, or a desiccated liver supplement, for their dense nutrient content including preformed vitamin A (retinol), zinc, and B vitamins.
- Leafy greens, seeds, and legumes for magnesium and B vitamins.
- Vitamin C-rich foods like bell peppers, citrus, strawberries, and kiwi — vitamin C is highly concentrated in the corpus luteum and supports its function.
Step 3: Stabilize Blood Sugar
Blood sugar dysregulation is one of the most underappreciated drivers of hormonal imbalance. When blood sugar spikes and crashes, insulin rises, which increases inflammation throughout the body — including in the ovaries. Prioritizing balanced meals (protein + fat + fiber + carbohydrate at every meal), avoiding long gaps between eating, and reducing ultra-processed foods are all practical first steps.
Step 4: Address Stress
Chronic stress directly suppresses the hypothalamic-pituitary-ovarian (HPO) axis — the communication pathway that triggers ovulation and drives progesterone production. Your body interprets prolonged stress as a sign that it is not safe to reproduce, and it will deprioritize ovulation accordingly. Sleep, nervous system support, and realistic stress reduction are not optional extras. They are foundational to fixing a short luteal phase.
Step 5: Support Gut Health
A healthier gut means better estrogen clearance, less ovarian inflammation, and better nutrient absorption — all of which support progesterone production. Practical steps:
- Stop drinking water at least 20 minutes before meals and wait about 30 minutes after, to avoid diluting stomach acid and digestive enzymes.
- Add digestive bitters before meals to support stomach acid production.
- Consider a digestive enzyme supplement to improve breakdown and absorption.
- Add 1 tablespoon of fermented foods (sauerkraut, kimchi, fermented vegetables) daily, or take a spore-based probiotic if fermented foods are not tolerated.
Step 6: Key Supplements for Corpus Luteum and Progesterone Support
These supplements work synergistically to support ovarian health and corpus luteum function. Give them a minimum of three to four menstrual cycles to see significant changes. Always consult your healthcare provider before starting new supplements, especially if you are on medications.
Vitamin C (500–1,000 mg daily) — Vitamin C is concentrated in the corpus luteum and has been shown in research to increase progesterone levels and protect the follicle and corpus luteum from oxidative stress. It is one of the most well-studied supplements for short luteal phase support. Split into two 500 mg doses if taking 1,000 mg.
Vitamin E (400–800 mg daily, as mixed tocopherols and tocotrienols) — Vitamin E is a powerful antioxidant that improves ovarian function, increases follicle health, and has been shown to enhance blood flow to the ovaries — all critical for better corpus luteum performance and progesterone output. Look for a supplement with mixed tocopherols, not just alpha-tocopherol alone.
Magnesium glycinate (200–400 mg daily) — Magnesium is essential for hundreds of biochemical reactions including mitochondrial function in the ovaries. It supports progesterone production, reduces inflammation, and is highly effective for cramping, PMS, sleep issues, and mood symptoms associated with luteal phase deficiency. Magnesium glycinate is gentle on the stomach and well absorbed. Topical magnesium spray is a good addition.
Vitamin A (as retinol via cod liver oil, 1 tsp daily) — Retinoids play a documented role in follicle development and ovarian steroid hormone production. Cod liver oil provides preformed vitamin A alongside vitamins D and K2, which all work together. Alternatively, eating liver 1–2 times a week achieves the same goal. Desiccated liver capsules are an option if you cannot tolerate liver.
Zinc (15–30 mg daily) — Zinc is critical for follicle development, ovulation, and corpus luteum function. It is also a key cofactor in progesterone synthesis. Many people with short luteal phases and low progesterone are zinc-deficient, particularly those who have been on hormonal birth control (which depletes zinc).
Shilajit (follow label dosing) — This trace mineral-dense resin supports mitochondrial function, which is especially important for the ovaries. It contains magnesium, calcium, zinc, iron, and fulvic acid (which improves mineral absorption). Think of it as a comprehensive remineralization supplement to support the energetic demands of the ovary.
B vitamins, especially B6 (25–50 mg daily) — Vitamin B6 is one of the most researched nutrients specifically for luteal phase deficiency. It is required for progesterone synthesis and helps lower elevated prolactin levels, which as we discussed, suppresses ovulation. B6 is also essential for dopamine synthesis, which indirectly supports the progesterone-prolactin axis. A B-complex is preferable to isolated B6 since B vitamins work together.
Step 7: Consider Vitex (Chasteberry)
If you have followed the dietary and supplement protocol consistently for 3–4 months and are still seeing a short luteal phase or persistent spotting, it is worth considering vitex (also known as chasteberry or chaste tree berry).
Vitex works by raising dopamine, which lowers prolactin levels. Lower prolactin means less suppression of LH, which supports ovulation and improves corpus luteum function — ultimately raising progesterone. It is particularly helpful for women who have recently come off hormonal birth control or who have borderline-elevated prolactin.
- Dosage: 500 mg in capsule form, taken in the morning on day 5 of your cycle through the first day of your next period. If you are not having regular periods, it can be taken continuously.
- Duration: 3–6 months minimum.
- Important caution: Vitex is a potent herb. It can cause mild nausea, acne, increased flow, or mood changes in some people. Use under the guidance of a practitioner if possible, and discontinue if you experience adverse effects.
Step 8: Castor Oil Packs
Castor oil packs applied to the lower abdomen 2–3 times per week support blood circulation to the ovaries and reproductive organs. Improved pelvic blood flow means better nutrient delivery to the ovaries and corpus luteum. This is a simple, inexpensive practice that complements everything else in this protocol.
Step 9: Bioidentical Progesterone (If Needed)
I want to be clear about something: supplemental progesterone should not be the first thing you reach for, and it should not be used without working on the underlying causes at the same time. Too many practitioners prescribe progesterone without ever investigating why it is low — and that approach leaves the root cause unaddressed.
That said, bioidentical progesterone can be a helpful tool, particularly if you are in perimenopause, experiencing recurrent miscarriage, or if the foundational work is in progress but symptoms are severe in the meantime. If you go this route:
- Only use it after ovulation has occurred (typically days 15–26 of a 28-day cycle, adjusted to your cycle). Using it before ovulation can suppress ovulation.
- Start low (5–10 mg topically) and increase gradually.
- Apply to rotating areas — inner thighs, lower abdomen, chest, wrists — to prevent tissue saturation.
- Work with a healthcare provider who can prescribe compounded bioidentical progesterone, which allows for precise dosing without synthetic fillers. Over-the-counter progesterone creams are a second option if prescription access is not available.
The goal is always to get your body producing adequate progesterone on its own. Supplemental progesterone is a support measure, not a permanent fix.
A Note on Timing and Patience
Healing a short luteal phase takes time. The follicle that will ovulate next month is already developing this month — and follicle development takes approximately 90 days from recruitment to ovulation. This means dietary and supplement changes made today will begin showing their full impact in your cycles roughly 3–4 months from now. That is not a reason to delay starting — it is a reason to be consistent and patient.
A realistic timeline is 1–2 months of healing for every year you have had symptoms. If your luteal phase issues have been going on for three years, expect meaningful improvement to take several months of consistent effort. That timeline can be shorter if you identify and address a specific root cause like thyroid dysfunction or a significant nutrient deficiency.
Get your personalized hormonal health protocol
Take the free Hormone Health Assessment — 30 questions about your cycle, symptoms, and lifestyle — and receive a tailored action plan built for your body.
Take the Free Assessment →