The Mirena IUD is one of the most widely used forms of hormonal contraception in the world — and one of the most misunderstood. It is frequently recommended not just for contraception, but for heavy periods, endometriosis, adenomyosis, and perimenopause management. Many providers describe it as a "low hormone" option that works almost entirely at a local level. And while that framing contains some truth, it glosses over a body of evidence showing that the Mirena does have measurable systemic effects — and that a meaningful subset of women experience real side effects because of them.
If you are considering the Mirena, currently have one, or are thinking about removal, this article will give you the full picture: how it works, what the research actually says about hormone levels, which side effects are underreported, who is likely to benefit, and what to do to support your body through the transition if you decide to remove it.
What Is the Mirena IUD?
The Mirena is a small, T-shaped plastic device that is placed inside the uterus by a healthcare provider. It releases a low daily dose of levonorgestrel — a synthetic progestin — directly into the uterine cavity. It is FDA-approved for up to 8 years of use, though it was previously approved for 5 years; current clinical guidelines now support extended use.
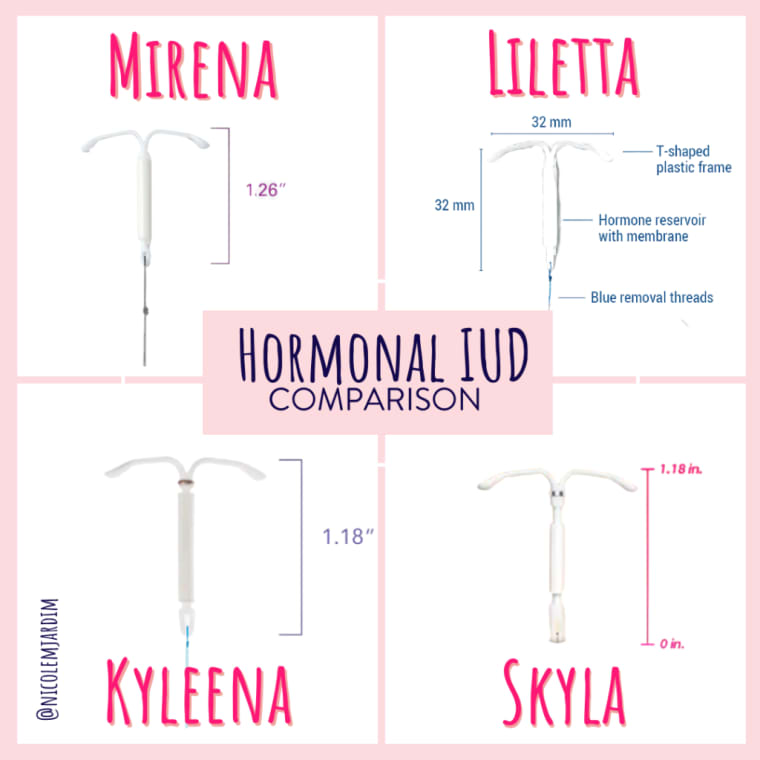
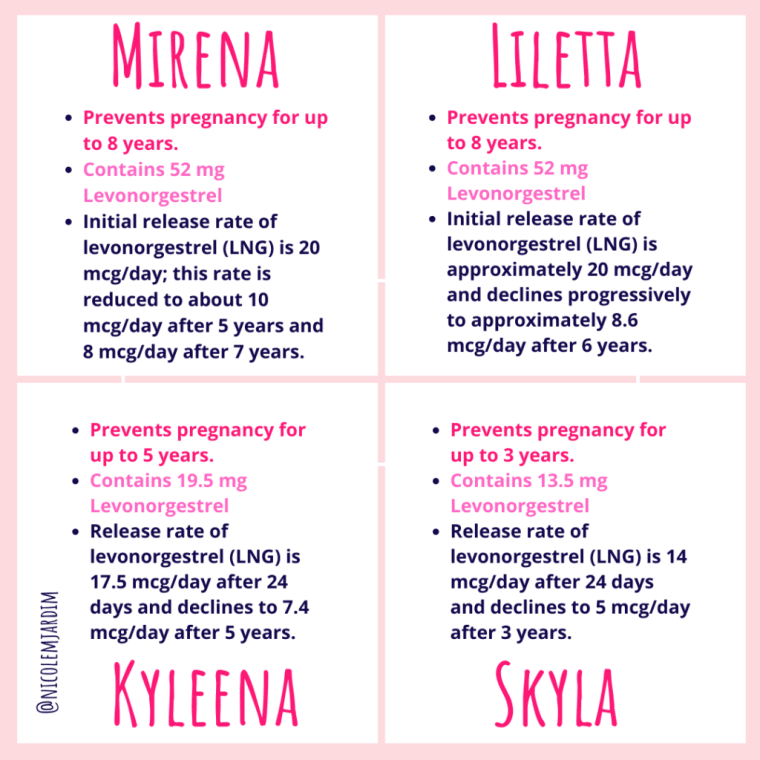
The Mirena is not the only hormonal IUD on the market. Kyleena, Liletta, and Skyla also release levonorgestrel, but at lower doses and with shorter licensed durations. Mirena releases the highest dose (approximately 20 micrograms per day initially, declining over time) and is the most studied device of its type.
Levonorgestrel is a second-generation progestin derived from testosterone. It has significant androgenic activity, meaning it binds not only to progesterone receptors but also to androgen receptors in the body. This is relevant to some of the side effects we will discuss shortly. For a deeper explanation of how synthetic progestins differ from natural progesterone, see my article on progestin vs progesterone.
How Does the Mirena Actually Work?
The Mirena prevents pregnancy through several overlapping mechanisms:
- Thickening cervical mucus so sperm cannot reach an egg — this is considered its primary contraceptive mechanism
- Thinning and suppressing the uterine lining (endometrium), making implantation less likely if fertilization does occur
- Inhibiting sperm motility via local changes in the uterine environment
- Suppressing ovulation in some users — this is not the primary mechanism, but studies show that ovulation is suppressed in roughly 50–75% of cycles in the first year of use, with ovulation more likely to resume in subsequent years
The key distinction between the Mirena and the combined pill or progestin-only pill is that the Mirena delivers hormone directly to the uterus, so the local concentration is very high while the systemic dose is much lower. This is the basis for the "local effect" claim.
Is It Really "Just Local"? What Research Says About Systemic Absorption
Here is where the conversation gets more nuanced than many providers let on. While levonorgestrel from the Mirena is delivered locally, it is not contained entirely to the uterus. Research consistently shows that measurable blood levels of levonorgestrel are present in Mirena users — they are simply lower than with oral or injected hormonal contraceptives.
Studies have found serum levonorgestrel levels in Mirena users ranging from approximately 50–150 picograms per milliliter, compared to the much higher levels seen with oral levonorgestrel pills. These systemic levels are low — but they are not zero. And for women who are particularly sensitive to androgenic progestins, even low systemic levels can be enough to cause noticeable effects.
Additionally, the Mirena suppresses ovulation in a significant proportion of users, particularly in the first year. This matters because when you do not ovulate, you do not produce the progesterone that follows ovulation. The downstream effects of low progesterone — mood changes, sleep disruption, anxiety, loss of the calming GABA-receptor effect that natural progesterone provides — can contribute to symptoms that users may not connect to their IUD.
The bottom line: the Mirena is lower-systemic than the pill or implant, but it is not a zero-hormone device. Individual response depends on how sensitive you are to levonorgestrel, whether ovulation is being suppressed, and your broader hormonal context.
How the Mirena Affects Your Cycle
One of the most commonly cited benefits of the Mirena is its effect on menstrual bleeding. For many women, this is genuinely transformative — particularly for those with heavy periods or bleeding conditions. Here is what typically happens:
- First 3–6 months: Irregular spotting, light bleeding between periods, and unpredictable cycle timing are very common and expected. This is the adjustment phase as the uterine lining thins.
- By 6–12 months: Periods typically become much lighter, shorter, and less painful. Many women also notice a reduction in cramping.
- At 1 year and beyond: Approximately 20% of Mirena users stop having periods altogether (amenorrhea). About 50% have significantly reduced flow. A smaller percentage continue to have irregular spotting throughout use.
The cessation or reduction of periods with the Mirena is caused by the thinning of the uterine lining — there is simply less tissue to shed. This is not the same as the natural process of menstruation, which is tied to a complete hormonal cycle including ovulation. If you are someone who tracks your cycle for health monitoring purposes or relies on your period as a vital sign of overall hormonal health, the loss of this feedback can feel disorienting — and it can mask underlying issues.
Side Effects Many Women Experience — But Don't Connect to Their IUD
The Mirena's product labeling includes a list of possible side effects, but many of the systemic complaints women report are often dismissed or attributed to other causes. Here are the side effects that are real, reported, and worth knowing about:
Mood Changes and Depression
A large Danish cohort study published in JAMA Psychiatry (2016) found a significantly increased risk of depression diagnosis and antidepressant use among hormonal IUD users compared to non-users — with the effect most pronounced in adolescents. Levonorgestrel does not have the same GABA-receptor activity as natural progesterone, meaning it does not provide progesterone's calming, anti-anxiety effect. Combined with the suppression of ovulation (and the natural progesterone it produces), some users experience worsening anxiety, low mood, or emotional numbness.
Decreased Libido
Low sex drive is a well-documented complaint among Mirena users and is likely multifactorial: lower circulating testosterone (progestins can reduce sex hormone-binding globulin in some users), suppressed ovulation (ovulation is a natural driver of libido), and direct effects of levonorgestrel on brain chemistry all play a role.
Hair Thinning and Acne
Because levonorgestrel has androgenic activity, it can bind to androgen receptors in the skin and hair follicles. Even at the lower systemic levels seen with the Mirena, women who are sensitive to androgens may experience increased hair shedding, thinning at the temples or crown, or acne — particularly along the jawline and chin. These symptoms are more common in women who already have a tendency toward androgenic symptoms.
Headaches and Migraines
Headaches are listed among the common side effects of the Mirena and are reported by a notable percentage of users. For women who are prone to hormonal migraines, the suppression of natural hormonal cycling — and particularly the loss of the mid-cycle estrogen peak associated with ovulation — can alter migraine patterns.
Cystic Ovaries (Ovarian Cysts)
Ovarian cysts are reported in approximately 12% of Mirena users. These typically form because ovulation is partially suppressed rather than fully blocked — follicles begin to develop but do not complete the process, and some persist as functional cysts. Most resolve on their own within a few months, but they can cause pelvic pain or discomfort.
Weight Changes
Weight gain is a commonly reported complaint. The mechanism is not entirely clear, but levonorgestrel's androgenic activity can affect fat distribution and may influence water retention in some users. Additionally, the disruption to natural hormonal cycling — including progesterone's role as a natural diuretic and fat-burning hormone — may contribute.
It is important to acknowledge that not every woman will experience these side effects. Many women use the Mirena for years with no significant complaints. But if you are experiencing any of the above and have a Mirena, it is worth having an honest conversation with your provider about whether the IUD may be a contributing factor — rather than immediately pursuing other diagnoses.
Not sure if your symptoms are hormone-related?
Take the free Hormone Health Assessment — 30 questions about your cycle, symptoms, and lifestyle — and get a personalized action plan built around your body.
Take the Free Assessment →Who Might Genuinely Benefit from the Mirena
Despite the side effects outlined above, there are specific situations where the Mirena offers meaningful clinical benefit — where the advantages can genuinely outweigh the risks:
Heavy Menstrual Bleeding
The Mirena is one of the most effective non-surgical treatments for heavy menstrual bleeding (menorrhagia). It reduces menstrual blood loss by 70–90% in most users by 12 months. For women whose heavy bleeding is causing anemia, fatigue, or significant disruption to daily life, this is a legitimate and evidence-backed benefit. The Mirena is often recommended as an alternative to endometrial ablation or hysterectomy.
Endometriosis
For women with endometriosis, the local progestogenic effect of the Mirena can suppress the growth of endometrial-type tissue and reduce painful periods. It is not a cure — it does not remove existing lesions — but it can be a helpful component of a comprehensive management plan, particularly for those who cannot tolerate or do not want systemic hormonal medications. Surgical excision remains the gold standard for diagnosis and treatment of endometriosis tissue, and the Mirena is typically most effective as an adjunct to, not a replacement for, excision surgery.
Adenomyosis
Adenomyosis — where endometrial-like tissue grows within the muscular wall of the uterus — is associated with heavy, painful periods and an enlarged uterus. The Mirena is one of the most effective non-surgical options for managing adenomyosis symptoms and is often recommended before considering a hysterectomy.
Perimenopause Management
For perimenopausal women who need uterine protection while taking estrogen therapy, the Mirena is an effective way to provide local endometrial protection — often without the systemic mood and cardiovascular effects of oral progestins. This is one of the most evidence-supported uses of the Mirena beyond contraception.
Who Might Reconsider or Have Higher Risk
The Mirena may not be the right choice — or may require extra consideration — for the following groups:
- Women with a personal or family history of depression, anxiety, or mood disorders — the risk of worsening symptoms is meaningful
- Women with existing androgenic tendencies (PCOS, hormonal acne, hair thinning) who may be more sensitive to levonorgestrel's androgenic activity
- Women with a history of hormonal migraines, which may worsen with suppression of the natural hormonal cycle
- Women who are planning to conceive in the near future — fertility typically returns quickly after removal, but the adjustment period can take a few months
- Women with uterine abnormalities, active pelvic infection, or unexplained vaginal bleeding, for whom IUD placement is not appropriate
- Women who strongly value having a regular, readable menstrual cycle as a health indicator — the Mirena makes this difficult to assess
Nutrient Depletion and Gut Microbiome Effects
This is an area that receives very little attention in standard IUD counseling, but it is worth understanding. The levonorgestrel released by the Mirena — even at lower systemic levels — is still a synthetic hormone processed by the liver, and it has effects on the gut and nutrient status similar to those seen with other hormonal contraceptives.
Research and clinical observation suggest that hormonal contraceptives, including progestin-releasing IUDs, can affect the following:
- Gut microbiome composition: Progestins can alter the diversity and balance of gut bacteria, which has downstream effects on immune function, mood (via the gut-brain axis), and the vaginal microbiome. Some women notice an increase in yeast infections or bacterial vaginosis while using hormonal IUDs.
- Intestinal permeability: Hormonal contraceptives have been associated with increased gut permeability — sometimes called "leaky gut" — which may contribute to inflammation, digestive symptoms, and immune dysregulation.
- B vitamins: Hormonal contraceptives can reduce circulating levels of B2, B6, B9 (folate), and B12 — all essential for energy, mood, red blood cell production, and reproductive health.
- Minerals: Magnesium, zinc, selenium, and phosphorus can all be depleted, affecting thyroid function, immune health, and ovarian function. Zinc in particular is critical for healthy ovulation and immune response.
- Vitamin C and E: Antioxidant levels may be reduced, increasing oxidative stress and inflammation.
The practical takeaway: if you have a Mirena, supporting your gut health, eating a nutrient-dense diet rich in B vitamins, zinc, and magnesium, and potentially supplementing strategically is worthwhile — not just after removal, but during use as well.
Thinking About Removal? A Recovery Protocol
Mirena removal is a straightforward in-office procedure that takes only a few minutes. What happens after removal is what women most often want to know about. Here is what to generally expect and how to support your body through the transition — the same principles that apply to coming off any hormonal contraceptive apply here. For a comprehensive guide, see my article on coming off birth control.
What to Expect After Removal
- Fertility typically returns within 1–3 months, though it can take longer for some women
- Periods will return, but they may initially be irregular or heavier than they were while on the Mirena as the uterine lining rebuilds
- If ovulation was suppressed, it may take several cycles to resume — this is especially true if you were using the Mirena for many years
- Some women experience a temporary return or worsening of the original symptoms the Mirena was managing (heavy bleeding, cramping) before the body recalibrates
Step 1: Prioritize Nutrition
Focus on a whole-foods diet that emphasizes the nutrients most likely to have been depleted: leafy greens and legumes for folate and B vitamins, pumpkin seeds and oysters for zinc, dark chocolate and leafy greens for magnesium, Brazil nuts for selenium, and brightly colored vegetables and citrus for vitamin C. Adequate protein is non-negotiable for hormone synthesis.
Step 2: Support Your Gut
Gut health is foundational to hormone clearance and production. Consider adding fermented foods (sauerkraut, kefir, kimchi), bone broth, and a high-quality probiotic. Digestive bitters before meals can help restore stomach acid production and improve overall digestive function. Reducing water intake during meals to avoid diluting digestive enzymes is also helpful.
Step 3: Replenish Minerals
Minerals are the spark plugs of hormonal health. Starting each morning with a pinch of sea salt in warm water, drinking bone broth regularly, and incorporating green juices (cucumber, celery, spinach, lemon) can meaningfully accelerate mineral restoration. An "adrenal cocktail" — combining vitamin C, sodium, and potassium — taken once or twice daily supports adrenal function and helps the body exit the chronic low-grade stress state that hormonal disruption can create.
Step 4: Support Liver Detoxification
The liver is responsible for clearing synthetic hormones and their metabolites. Supporting detoxification pathways through cruciferous vegetables (broccoli, Brussels sprouts, kale), adequate hydration, and reducing the toxic load in your home environment (switching to natural cleaning products, filtering water) all reduce the burden on the liver during the transition period.
Step 5: Key Supplements to Consider
The following supplements have strong rationale for post-IUD support. Always work with a practitioner to determine what is right for your individual situation:
- Magnesium glycinate (100–400 mg daily): supports adrenal function, sleep, mood, and muscle relaxation — one of the most commonly depleted minerals in hormonal contraceptive users
- B-complex or methylated B vitamins: restore B2, B6, B12, and folate levels; particularly important if you have MTHFR gene variants that affect folate metabolism
- Zinc: essential for ovulation, immune function, and skin health; often depleted by progestin use
- A quality multivitamin or desiccated beef liver capsules as a broad-spectrum nutrient insurance policy
- Adaptogenic herbs (ashwagandha, holy basil): support the HPA axis and adrenal recovery, reduce cortisol, and improve stress resilience during hormonal transition
- Probiotics: to restore microbiome diversity disrupted by hormonal contraceptive use
When to See a Doctor
Contact your healthcare provider promptly if you experience any of the following while using the Mirena:
- Severe pelvic pain or cramping, especially if sudden in onset
- Pain during sex that is new or worsening
- Fever, chills, or unusual vaginal discharge (signs of possible infection)
- You cannot feel the IUD strings during self-check (or your partner notices the hard plastic)
- Positive pregnancy test — rare but possible with IUDs, and ectopic pregnancy risk is elevated
- Significant mood changes, worsening depression, or suicidal thoughts
- Partial expulsion or unusual cramping that suggests the device may have moved
For any concerns about whether the Mirena is right for your specific situation — including if you have a history of mood disorders, PCOS, endometriosis, or are considering it during perimenopause — work with a provider who will take your full hormonal history into account.
A Note on Insertion and Removal Conversations
IUD insertion can be painful, and the level of discomfort varies widely — some women find it manageable, while others experience significant cramping during and after the procedure. You are fully entitled to ask your provider in advance about pain management options, including topical anesthesia, a cervical block, or pre-procedure NSAIDs. "Just relax" is not adequate pain management for everyone, and advocating for your comfort during this procedure is reasonable and appropriate.
Removal is generally much quicker and less painful than insertion. If your provider encounters difficulty (e.g., strings are not visible), a minor procedure with ultrasound guidance may be required. This is not uncommon and is not a cause for alarm.
The Bottom Line
The Mirena IUD is a genuinely useful tool in the right context. For heavy bleeding, endometriosis, adenomyosis, and certain perimenopausal needs, it offers evidence-backed benefits that can be life-changing. But it is not a zero-hormone, side-effect-free device — it releases a testosterone-derived synthetic progestin that does reach systemic circulation, can suppress ovulation, and can affect mood, libido, skin, hair, and gut health in ways that are real and underreported.
The most important thing is to make an informed decision: understand how it works, know your own hormonal history and sensitivities, and have a provider who listens if something does not feel right. Your body's response to any hormonal contraceptive is valid data — not something to dismiss or push through indefinitely.